

Ready or not...here are 13 more jokes to make you groan!
1. Patient: "What’s that floater doing in my eye, doctor?" Doctor: “The sidestroke.”
2. Doctor: “Have your eyes ever been checked before?” Patient: “No, they’ve always been hazel.”
3. Why did the cyclops have to close his school? He had only one pupil!
4. Why wouldn’t the optometrist learn any jokes? He had heard that a joke can help break the eyes.
5. What is it called when you poke your eye with safety glasses? Eye-rony!
6. Did you here about the new website for people with chronic eye pain? It’s a site for sore eyes.
7. When are your eyes not eyes? When an onion makes them water!
8. Why do beekeepers have such beautiful eyes? Because beauty is in the eye of the bee holder!
9. Why were the teacher’s eyes crossed? Because she couldn’t control her pupils.
10. What's your eye doctor's favorite treat? Candy cornea!
11. What has four eyes and a mouth? The Mississippi.
12. Did you know that your left eye isn't real? It's just in your head.
13. What did the optometrist say when the patient complained he made too many jokes? “Bad puns are how eye roll.”
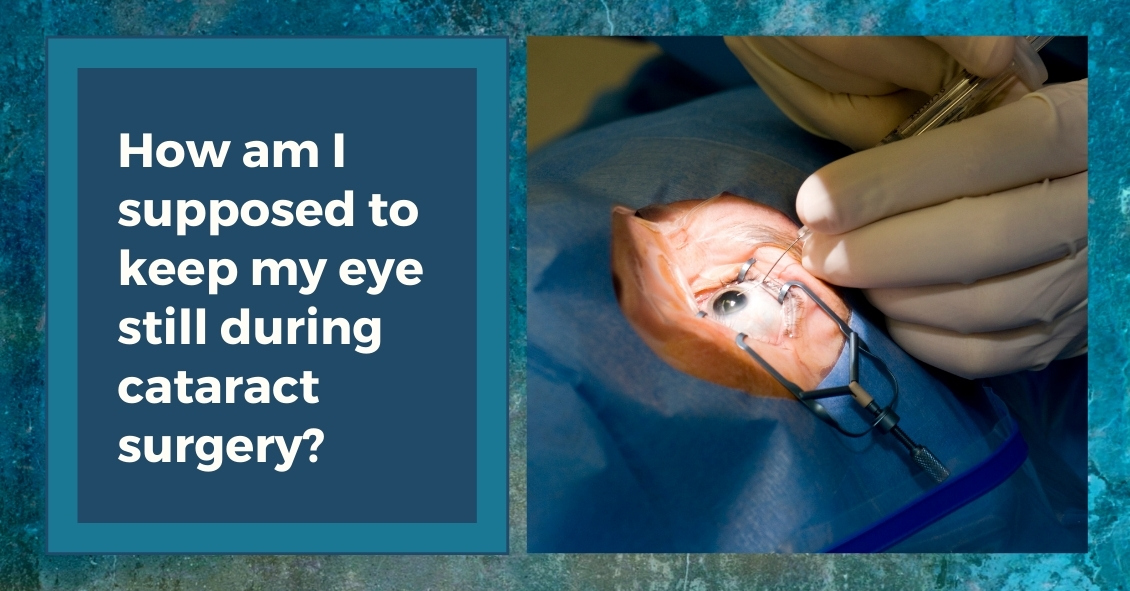
The majority of cataract surgeries performed in the U.S. are done with a local anesthetic and IV sedation.
The local anesthesia may be accomplished in one of two ways: either an injection of anesthetic around the eye or anesthetic eye drops placed on the eye, often combined with an injection of a small amount of anesthetic into the front of the eye at the very beginning of surgery.
The injection of anesthetic around the eye generally produces a deeper anesthesia for the surgery than the topical method but it also comes with increased risk. There is a very small chance of potentially serious bleeding behind the eye and a rare chance of inadvertent penetration of the back of the eye with the injection needle.
The topical anesthesia has lower risk but does not provide quite as deep of an anesthesia, although the overwhelming majority of people having cataract surgery with a topical anesthetic do not experience any significant pain during the procedure.
The other difference between the two anesthesias is that with topical anesthesia you maintain your ability to move your eye around whereas with injection anesthesia the eye muscles are temporarily paralyzed so your eye doesn’t move during the surgery. When you have topical anesthesia it is important for you to try to stare straight ahead at the light in the microscope above you. Most people accomplish this quite easily.
Along with the anesthetic to the eye, in most cataract surgeries an anesthetist will also give you some mild sedative medication through an IV. This relaxes you but does not put you “out,” although some people do fall asleep during the procedure from the effects of the sedation.
Many people who have cataract surgery with IV sedation don’t remember some of the surgery because of the amnesiac effect that occurs from the sedative. This often doesn’t happen when you return for surgery on your second eye.
Despite often getting the exact same dose of sedative on the second surgery you have significant less amnesia the second time. This is caused by a quick buildup in tolerance to the medication.
When they have their second surgeries, many patients feel that the surgery was significantly different than the first time even though it was done exactly the same. The reason is just that you remember more the second time.
On rare occasions people need to have general anesthesia to have their cataracts removed. Today, that is mostly done for people who are incapable of cooperating and staying still for the surgery. For everyone who can cooperate it is generally not worth the risks, which include death, to put people to sleep for a surgery that is easily done under a local anesthetic.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Read more: What Anesthesia Might You Have for Cataract Surgery?
What Is Intraoperative Aberrometry?
Yes, that is a mouthful, but the concept isn’t quite as hard as the name.
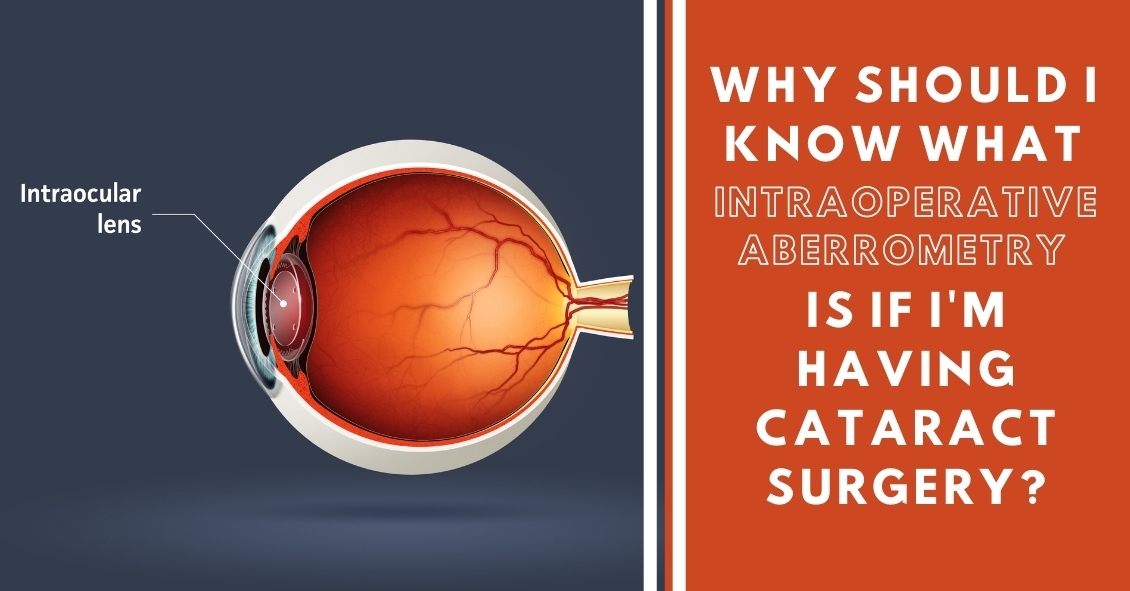
An Intraoperative Aberrometer is an instrument we can use in the operating room to help us determine the correct power of the implant we put in your eye during cataract surgery.
Cataract surgery is the removal of the cloudy natural lens of your eye and the insertion of a new artificial lens inside your eye called an intraocular lens (IOL).
The cloudy cataract that we are removing has focusing power (think of a lens in a camera) and when that lens is removed, we need to insert an artificial lens in its place to replace that focusing power. The amount of focusing power the new IOL needs has to match the shape and curvature of your eye.
To determine what power of lens we select to put in your eye, we need to measure the shape and curvature of your eye prior to surgery. Once we get those measurements, we can plug those numbers into several different formulas to try and get the most accurate prediction of what power lens you need.
Overall, those measurements and formulas are very good at accurately predicting what power lens you should have. There are, however, several eye types where those measurements and formulas are less accurate at predicting the proper power of the replacement lens.
Long Eyes: People who are very nearsighted usually have eyes that are much longer than average. This adds some difficulty with the accuracy of both the measurements and the formulas. There are special formulas for long eyes but even those are less accurate than formulas for normal length eyes.
Short Eyes: People who are significantly farsighted tend to have shorter-than-normal eyes. Basically, the same issues hold true for them as the ones for longer eyes noted above.
Eyes with previous refractive surgery (LASIK, PRK, RK): These surgeries all change the normal shape of the cornea. This makes the formulas we use on eyes that have had previous surgery not work as well when the normal shape of the cornea has been altered.
This is where intraoperative aberrometry comes in. The machine takes the measurements that we do before surgery and then remeasures the eye while you are on the operating room table after the cataract is removed and before the new implant is placed inside the eye. It then presents the surgeon with the power of the implant that the aberrometer thinks is the correct one. Unfortunately, the power that the aberrometer selects isn’t always exactly right, but with the combination of the pre-surgery measurements and the intra-surgery measurements the overall accuracy is significantly enhanced.
The intraoperative aberrometry is also very helpful in choosing the power of specialty lenses like multi-focal and toric lenses.
We would encourage you to consider adding intraoperative aberrometry to your cataract surgery procedure if you have either a long or short eye (usually manifested as a high prescription in your glasses) or if you have had any previous refractive surgery.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Read more: Why Should I Know What Intraoperative Aberrometry Is?
In our modern world, people spend hours on end staring at computer screens, smartphones, tablets, e-readers, and books that require their eyes to maintain close focus.
For most people (all except those who are nearsighted and aren’t wearing their glasses), their eyes’ natural focus point is far in the distance. In order to move that focus point from far to near, there is an eye muscle that needs to contract to allow the lens of the eye to change its shape and bring up-close objects into focus. This process is called accommodation.
When we accommodate to view close objects, that eye muscle has to maintain a level of contraction to keep focused on the near object. And that muscle eventually gets tired if we continuously stare at the near object. When it does, it may start to relax a bit and that can cause vision to intermittently blur because the lens shape changes back to its distance focal point and the near object becomes less clear.
Continuing to push the eyes to focus on near objects once the focus starts to blur will began to produce a tired or strained feeling in addition to the blur. This happens very frequently to people who spend long hours reading or looking at their device screens.
An additional problem that occurs when we stare at objects is that our eyes’ natural blink rate declines. The average person blinks about 10 times per minute (it varies significantly by individual) but when we are staring at something our blink rate drops by about 60% (4 times per minute on average). This causes the cornea (the front surface of the eye) to dry out faster. The cornea needs to stay moist in order to see clearly, otherwise little dry spots start appearing in the tear film and the view gets foggy. Think about your view through a dirty car windshield and how much that view improves when you turn the washers on.
So what should you do if your job, hobby, or passion requires you to stare at a close object all day?
Follow the 20-20-20 rule. Every 20 minutes, take 20 seconds and look 20 feet into the distance. This lets the eye muscle relax for 20 seconds, and that is generally enough for it to have enough energy to go back to staring up close for another 20 minutes with much less blurring and fatigue. It also will help if you blink slowly several times while you are doing this to help re-moisten the eye surface.
Don’t feel like you can give up those 20 seconds every 20 minutes? Well if you don’t, there is evidence that your overall productivity will decline as you start suffering from fatigue and blurring. So take the short break and the rest of your day will go much smoother.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Nowdays, many people prefer shopping online to shopping in stores for many of their needs.
With technology constantly improving and evolving, people like the convenience of shopping online. Whether it’s clothing, electronics, or even food, you can easily find almost everything you need on the Internet.
Eyeglasses, unfortunately, are no different. Many online shops have been popping up in recent years, offering people that same convenience. But what they don’t tell you is that it comes at a price, and this article’s purpose is to shine a light on the negatives of shopping online for eyeglasses.
Here are some important reasons to avoid the temptation of ordering glasses online.
- Accuracy- Instead of saving the most important point for last, we will focus on the main reason that ordering eyeglass online is not the best choice. Product accuracy is a huge reason that the online market has not completely taken off. Every person who needs eyeglasses needs to understand the process for how their prescription is obtained in order to truly understand why shopping online is not ideal. It is called an eyeglass prescription for a reason. Your ophthalmologist or optometrist is prescribing your lenses as if they were prescribing any form of medication. To take that prescription and hand it over to a website that does not require licensed workers to interpret the prescription is not the wisest choice. Equally as important as the prescription itself are the pupillary distance (PD) and the optical centers measurements. These measurements are not given at the time of the examination by the eye doctor, but instead are administered by the optician at the point of sale. Not having these measurements done accurately will negatively affect the quality of vision as much as an error in the prescription.
- Quality- The quality of the product you are purchasing is often affected when making the decision to purchase online. Websites rely on low overhead, high volume, and lack of quality control. The online experience pales in comparison to the quality you will receive in a professional office. Skilled opticians who interpret and manufacture your eyeglass prescriptions are generally held to a much higher standard than an online website.
- Warranty- Due to their low prices, many of these websites do not include much in the way of product warranty or guarantee. Local eyecare practices, however, stand behind your purchase. If there are issues with adjustment or a patient not being comfortable in a specific lens or product, professional optometrists and opticians are willing to work with you. This personal experience is not attainable on the web.
- Coordination with Your Doctor- With the complexity of eyeglass lenses, the ease of working in house is always a benefit worth keeping in mind. Eyeglass lenses can be very complex products. Having the benefit of being able to work directly with the doctor gives the optician the best chance to put you in the exact lenses you need. There is a substantial difference in the percentage of error between shopping online and the care you get in a private practice.
- Personal Experience- The biggest factor for many people is that the customized experience you get when shopping in person is something you cannot obtain by using the Internet. Dealing with the same opticians year in and out is something patients emphasize and appreciate. Just like people tend to keep the same doctors over the years, patients like knowing that the same people will be in charge of making/ordering their glasses. Shopping online will not offer that experience.
All of these factors should be carefully weighed when making the decision to shop online. While the initial price difference could entice you at first, know that it does come at a price. Whether it be a warranty, quality, or convenience issue, all of these are very important factors when buying glasses. People sometimes tend to discount how intricate eyeglasses are.
Purchasing eyeglasses is handled best in person by professionals who can provide you with the utmost care and quality.
Article contributed by Richard Striffolino Jr.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Dry Eye Disease affects more than 5 million people in the United States, with 3.3 million being women and most of those being age 50 or over. And as people live longer, dry eye will continue to be a growing problem.
Although treatment options for dry eyes have improved recently, one of the most effective treatments is avoidance of dry eye triggers.
For some that might mean protecting your eyes from environmental triggers. To do that experts recommend using a humidifier in your home, especially if you have forced hot-air heat; wearing sunglasses when outside to help protect your eyes from the sun and wind that may make your tears evaporate faster; or being sure to direct any fans - such as the air vents in your car - from blowing directly on your face. For others, it may mean avoiding medications that can cause dry eyes.
There is one other trigger that may need to be avoided that doesn’t get as much notice: the potentially harmful ingredients in cosmetics.
Cosmetics do not need to prove that they are “safe and effective” like drugs do. The FDA states that cosmetics are supposed to be tested for safety but there is no requirement that companies share their safety data with the FDA. There are also no specific definition requirements for labeling cosmetics as “hypoallergenic,” “dermatologist tested,” “ophthalmologist tested,” “sensitive formula” or the like, making most of those labels more marketing than science.
Things to watch out for in your cosmetics if you have dry eye include:
Preservatives
Preservatives are important to prevent the cosmetics from becoming contaminated but many are known to exacerbate dry eye. Common preservatives in cosmetics that could be adding to your dry eye problems (Periman and O’Dell, Ophthalmology Management August 2016) are: BAK (Benzalkonium chloride); Formaldehyde-donating (yes, Formaldehyde!) preservatives (often listed as DMDM-hydantoin, quaternium-15, imidazolidinyl urea, diazolidinyl urea and 2-bromo-2-nitropropane-1,3-diol); parabens; and Phenoxyethanol. All of these preservatives in sufficient quantities can cause ocular irritation or inhibit the function of the Meibomian Glands that produce mucous that coats your tear film and keeps it from evaporating too quickly.
Alcohol
Alcohol is used in cosmetics mostly to speed the drying time but the alcohol can also dry the surface of the eye.
Waxes
Waxes can block the opening of the Meibomian Glands along the eyelid margin. If these glands are blocked they will not be able to supply the mucous and lipids necessary to the tear film to prevent it from drying too quickly. If you have trouble with dry eye it would be advisable not to apply eye liner behind the eyelashes along the lid edge where the Meibomian gland openings are.
Anti-aging products
While these may be safe and effective for the skin of the face they should not be used around the eyes. Most of these products contain some form of Retin A. These products have been shown to be toxic to the Meibomian glands and could be contributing to your dry eyes.
These components of cosmetics do not adversely affect everyone. However, if you suffer from dry eye and are not effectively able to keep your eye comfortable and your vision clear, you should investigate your cosmetics as a potential contributor to your problem.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Living an overall healthy life is good for your eyes. Healthy vision starts with healthy eating and exercise habits.
There's more to complete eye health than just carrots. Are you eating food that promotes the best vision possible? Learn what foods boost your eye well-being and help protect against diseases. Here are important nutrients to look for when selecting your foods.
- Beta carotene or Vitamin A (helps the retina function smoothly): carrots and apricots
- Vitamin C (reduce risk of macular degeneration and cataracts): citrus and blueberries
- Vitamin E (hinders progression of cataracts and AMD): almonds and sunflower seeds
- Riboflavin (helps your eyes adapt in changes in light): broccoli and bell peppers
- Lutein (antioxidant to maintain health while aging): spinach and avacado
- Zinc (transfers vitamin A to the retina for eye-protective melanin productions and helps with night vision): beans and soy beans
- DHA (helps prevent Dry Eye): Fatty fish like salmon and tuna
Keep in mind, cooked food devalues the precious live enzymes, so some of these foods are best eaten raw.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Sunglasses are more than just a fashion statement - they’re important protection from the hazards of UV light.
If you wear sunglasses mostly for fashion that’s great--just make sure the lenses block UVA and UVB rays.
And if you don’t wear sunglasses, it’s time to start.
Here are your top 6 reasons for wearing sunglasses:
#1--Preventing Skin Cancer
One huge way that sunglasses provide a medical benefit is in the prevention of skin cancer on your eyelids. UV light exposure from the sun is one of the strongest risk factors for the development of skin cancers.
Each year there are more new cases of skin cancer than the combined incidence of cancers of the breast, prostate, lung and colon.
About 90 percent of non-melanoma skin cancers are associated with exposure to ultraviolet (UV) radiation from the sun.
Your eyelids, especially the lower eyelids, are also susceptible to UV light and they do develop skin cancers somewhat frequently.
Many people who now regularly apply sunscreen to help protect them from UV light often don’t get that sunscreen up to the edge of their eyelids because they know the sunscreen is going to make their eyes sting and burn. Unfortunately, that leaves the eyelids unprotected. You can fix that by wearing sunglasses that block both UVA and UVB rays.
#2--Decreasing Risk For Eye Disease
There is mounting evidence that lifetime exposure to UV light can increase your risk of cataracts and macular degeneration. It also increases your risk of getting growths on the surface of your eye called Pinguecula and Pterygiums. Besides looking unsightly, these growths can interfere with your vision and require surgery to remove them.
#3--Preventing Snow Blindness
Snow reflects UV light and on a sunny day the glare can be intense enough to cause a burn on your cornea--much like what happens when people are exposed to a bright welding arc.
#4--Protection From Wind, Dust, Sand
Many times, when you are spending time outdoors and it is windy, you risk wind-blown particles getting into your eyes. Sunglasses help protect you from that exposure. The wind itself can also make your tears evaporate more quickly, causing the surface of your eye to dry out and become irritated, which in turn causes the eye to tear up again.
#5--Decreasing Headaches
People can get headaches if they are light sensitive and don’t protect their eyes from bright sunlight. You can also bring on a muscle tension headache if you are constantly squinting because the sunlight is too bright.
#6--Clearer Vision When Driving
We have all experienced an episode of driving, coming around a turn, looking directly into the direction of the setting or rising sun, and having difficulty seeing well enough to drive safely. Having sunglasses on whenever you are driving in sunlight helps prevent those instances. Just a general reduction in the glare and reflections that sunlight causes will make you a better and more comfortable driver.
So it’s time to go out there and find yourself a good pair of sunglasses that you look great in and that protect your health, too.
Your eye-care professional can help recommend sunglasses that are right for your needs.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Need a chuckle or a groan? Here you go...
1. Did you hear about the guy who just found out he was color blind? It hit him right out of the purple!
2. What happened to the lab tech when he fell into the grinder? He made a spectacle of himself.
3. Why is our staff so amazing? They were all bright pupils!
4. Why did the smartphone have to wear glasses? It lost all of its contacts.
5. What did one pupil say to the other? I’m dilated to meet you.
6. What do you call a potato wearing glasses? A Spec-Tater!
7. What do you call an optician living on an Alaskan island? An optical Aleutian.
8. What was the innocent lens’s excuse to the policeman? "I’ve been framed, officer!"
9. Where is the eye located? Between the H and the J.
10. Where does bad light end up? In Prism!

Is it safe to use "Redness Relief" eye drops regularly?
The short answer is NO.
Here’s the slightly longer answer.
There are several eye “Redness Relief” products on the over-the-counter market, such as those made by Visine, Clear Eyes, and Bausch & Lomb - as well as generic versions sold by pharmacy chains.
Most commonly, the active ingredient in redness relief drops is either Tetrahydrozoline or Naphazoline. Both of these drugs are in a category called sympathomimetics.
Sympathomimetics, the active ingredient in redness relief drops, work though a process called vasoconstriction, an artificial clamping down of the superficial blood vessels on the eye surface. These blood vessels often dilate in response to an irritation. This increase in blood flow is trying to help repair whatever irritation is affecting the surface of the eye. Clamping down on those vessels by using a vasoconstrictor counteracts the body’s efforts to repair the problem.
The other downside to repetitively using redness relief drops is that after the vasoconstrictor wears off the vessels often dilate to an even larger degree than when the process started. This stimulates you to use the drops again.
All of these drops carry these same two warnings on their labels:
Do not overuse as it may produce increased redness of the eye.
Stop using and ask a doctor if you experience eye pain, changes in vision, continued redness or irritation of the eye condition worsens or persists for more than 72 hours.
Does anyone read those warnings? Almost never.
These drops are meant to be used for a VERY short duration - one or two days. That’s it!
They are not meant to be used indefinitely and they are certainly not meant to be used daily.
Take a good look at that first warning: MAY PRODUCE INCREASED REDNESS OF THE EYE.
If you are using redness relief drops repetitively you are likely making your eye redness WORSE, not better.
If you have been using redness relief drops daily you need to stop and replace them with an artificial tear or lubricating drop - something that DOES NOT say “gets the red out.”
After you make that switch your eyes are initially going to be red as your blood vessels take time to regain their normal vascular tone without the vasoconstrictor clamping down on them. The lubricating drop will actually help to repair the damage done by exposure to adverse conditions. This will decrease the inflammatory signals that make the vessels dilate. You will actually be doing something helpful to the surface of your eyes instead of just masking everything by artificially clamping down on your vessels and decreasing the flow of oxygen and nutrients to the front surface of your eye.
Using redness relief drops if you wear contacts is an even worse idea. If you put the drop in with your contact in, the contact will hold onto the drug and keep it on your eye surface longer, thus likely increasing the vasoconstriction.
Your cornea has no blood vessels in it and it depends on the blood vessels in the conjunctiva over the whites of the eye to bring in nutrients and oxygen. The other source of oxygen for the cornea is what it gets from diffusion from the atmosphere and that is also cut down by the presence of the contact lens.
The redness relief drop combined with the contact lens are now BOTH reducing the levels of oxygen getting to the cornea. Decreased oxygen to the cornea is one of the biggest risks for contact lens-related infections, including corneal ulcers.
Don’t get me wrong, I’m not condemning redness relief drops if used appropriately for a very short time to soothe the eyes if they have been temporarily exposed to elements that made them irritated. For a day or two redness relief drops are fine. But for long-term use or for use while wearing your contacts they are much more likely to cause problems than to provide any benefits.
Article contributed by Dr. Brian Wnorowski, M.D
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

We all know that during pregnancy, a woman's body goes through a great deal of change hormonally and physiologically. But did you know her eyes change as well? Below are some of the most common effects pregnancy can have on the eye.
- Corneal changes. In some cases, pregnancy can cause the cornea, the front window of the eye, to change curvature and even swell, leading to shifts in glasses and contact lens prescriptions. In addition, changes in the chemistry of the tear film can lead to dry eyes and contact lens intolerance. It is for these reasons that it is generally not recommended to have any new contact lens fitting or new glasses prescription checks until several months postpartum. We want to get the most accurate measurements possible.
- Retinal changes. Many different conditions can affect the retina during pregnancy. If the pregnant woman has diabetes, diabetic eye disease can progress by 50%. In women with preeclampsia, a condition where blood pressure rises significantly, over 40% of women can show changes in the retinal blood vessels, and 25% to 50% complain of changes to their vision.
- Eye Pressure Fluctuation. Intraocular pressure (IOP) usually decreases during pregnancy. The exact mechanism causing this is unknown, but it is usually attributed to an increase of flow of intraocular fluid out of the eye. This is good news for pregnant women with glaucoma or high IOP. In fact, the drop in IOP is larger when you start with a high IOP compared to one in the normal range.
There are many more effects that pregnancy can have on the eye, but these are the most common. One other thing to keep in mind is that though the likelihood of any adverse effect is extremely low, we try not to use any diagnostic eye drops on pregnant patients during the eye exam. Unless there is a medical necessity to dilate the pupils or check IOP, it is a good rule of thumb to put off using drops until after the patient has given birth in order to protect the developing baby.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Alzheimer's Disease International estimates that the number of people living with dementia worldwide - nearly 44 million in 2014 - will almost double by 2030 and more than triple by 2050.
There is no single test that can show if a person has Alzheimer's, but doctors can almost always determine if a person has dementia, although it may be difficult to determine the exact cause. Diagnosing Alzheimer's requires careful medical evaluation, neurological testing, and sometimes brain imaging and blood tests to rule out other causes of dementia.
Most of the testing for early disease - MRI scans of the brain, brain PET scans looking for amyloid, and spinal taps looking for certain proteins in the spinal fluid - are not very accurate, and they are invasive and often expensive.
Researchers have now turned to findings in the eye to help with early detection and are hoping to find ways to make the diagnosis earlier when potential treatments may have a better outcome. There is also hope that these tests will be less expensive and invasive then the other options.
One of the tests that has shown promise is an OCT of the retina. Almost every eye doctor’s office already has an OCT, and so if this research proves fruitful, the test could be done relatively cheaply because there is not a need to buy more expensive equipment. The average OCT exam costs much, much less than the cost of an MRI or PET Scan.
Neuroscientists at the Gladstone Institutes in San Francisco showed a proof of concept in frontotemporal dementia, which is like Alzheimer’s but attacks much earlier and accounts for just 10% to 15% of dementia cases. They found that patients with frontotemporal dementia had thinning of the neuron layer of the retina on OCT.
In a study at Moorfields Eye Hospital they also found that people who had a thinner layer of neurons in the macula on an OCT exam were more likely to perform poorly on the cognitive tests - a clear warning sign they may be undergoing the early stages of dementia.
Study leader Dr. Fang Ko, said: “Our findings show a clear association between thinner macular retinal nerve fiber layer and poor cognition in the study population. This provides a possible new biomarker for studies of neurodegeneration.”
A second marker that is getting a careful look is identifying the presence of amyloid in the eye. Amyloid, thought to be one of the key causes of Alzheimer’s, which makes up most dementia cases, is often found to have formed into clumps and plaques in the brain. Scientists at Waterloo University in Canada found people with severe Alzheimer’s disease had deposits of a protein amyloid on their retinas.
Research conducted at Lifespan-Rhode Island Hospital in Providence co-led by Peter Snyder, a professor of neurology at Brown University, and Cláudia Santos, a graduate student at the University of Rhode Island, is attempting to detect amyloid in the retina by OCT and follows people over time to see if the amyloid increases and if it correlates with cognitive impairment.
Another angle being pursued by a company called Cognoptix is looking for amyloid in the lens of the eye. Using Cognoptix's SAPPHIRE II system, which detects amyloid in the lens, a 40-person Phase 2 clinical trial was conducted at four sites. The study recruited patients who were clinically diagnosed with probable Alzheimer’s disease (AD) via a rigorous neuropsychological and imaging workup. The study, using age-matched healthy controls, showed outstanding results of 85% sensitivity, and 95% specificity in predicting which people had probable AD.
The company planned a Phase 3 study that must show a strong correlation in a bigger study group to obtain ultimate FDA approval.
One of the other items I was going to include in this post was information on what visual symptoms occur in dementia patients and how family and friends can support them but I found an outstanding review already available online by the Alzheimer’s society that covers all those points. If you have a loved one with dementia this is an excellent read and I highly recommend you take the time to review it.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

When soft contact lenses first came on the scene, the ocular community went wild.
People no longer had to put up with the initial discomfort of hard lenses, and a more frequent replacement schedule surely meant better overall health for the eye, right?
In many cases this was so. The first soft lenses were made of a material called HEMA, a plastic-like polymer that made the lenses very soft and comfortable. The downside to this material was that it didn’t allow very much oxygen to the cornea (significantly less than the hard lenses), which bred a different line of health risks to the eye.
As contact lens companies tried to deal with these new issues, they started to create frequent-replacement lenses made from SiHy, or silicone hydrogel. The oxygen transmission problem was solved, but an interesting new phenomenon occurred.
Because these were supposed to be the “healthiest” lenses ever created, many people started to overwear their lenses, which led to inflamed, red, itchy eyes; corneal ulcers; and hypoxia (lack of oxygen) from sleeping in lenses at night. A new solution was needed.
Thus was born the daily disposable contact lens, which is now the go-to lens recommendation of most eye care practitioners.
Daily disposables (dailies) are for one-time use, and therefore there is negligible risk of overwearing, lack of oxygen, or any other negative effect that extended wear (2-week or monthly) contacts can potentially have. While up-front costs of dailies are higher than their counterparts, there are significant savings in terms of manufacturer rebates. In addition, buying contact lens solution is no longer necessary!
While a small minority of patient prescriptions are not yet available in dailies, the majority are--and these contacts have worked wonders for patients who have failed in other contacts, especially those who have dry eyes.
Ask your eye care professional if dailies might be the right fit for you.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

What’s up with people wearing those big sunglasses after cataract surgery?
The main reason is for protection - physical protection to assure nothing hits the eye immediately after surgery, and protection from sunlight and other bright lights.
We want to protect the eye from getting hit physically because there is a small incision in the eyeball through which the surgeon has removed the cataract and inserted a new clear lens. In most modern cataract surgeries that incision is very small - about one-tenth of an inch in most cases. The vast majority of surgeons do not stitch the incision closed at the end of surgery. The incision is made with a bevel or flap so that the internal eye pressure pushes the incision closed.
The incision does have some risk of opening, especially if you were to provide direct pressure on the eyeball. Therefore, immediately after surgery we want you to be careful and make sure that you or any outside force doesn’t put direct pressure on the eye. The sunglasses help make sure that doesn’t happen while you are outside immediately after surgery. It’s the same reason that most surgeons ask you to wear a protective plastic shield over the eye at night while you are sleeping for the first week so that you don’t inadvertently rub the eye or smash it into your pillow.
The other advantage of wearing the sunglasses is to protect your eye from bright light, especially in the first day or two when your pupil may still be fairly dilated from all the dilating drops we used prior to surgery. Even after the dilation wears off, the light still seems much brighter than before your surgery. The cataracts act like internal sunglasses. The lens gets more and more opaque as the cataract worsens and so it lets less and less light into the eye. Your eye gets used to those decreased light levels and when you have cataract surgery the eye instantly goes from having all the lights dimmed by the cataract to 100% of the light getting through the new clear lens implant. That takes some getting used to and the sunglasses help you adapt early on. Think of this as if you were in a dark cave for a long period of time and then were thrust out into the bright sunlight. It would be pretty uncomfortable. The sunglasses help with that adjustment.
So why do people keep wearing those sunglasses long after their surgery? Mostly because some people really like them. They not only provide sun protection straight on, they also give you protection along the top and sides of the frame, reducing the light that can enter around the frame
If you have a spouse who wants to keep wearing those...let’s call them “inexpensive” and “less than fashionable”...sunglasses, but you’d like them to look better, there is a solution. There are sunglasses called Fitovers that go over top of your regular glasses and still provide top and side protection from the sun but look much better than the “free” ones you got for cataract surgery.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Read more: What Is the Deal with Those Weird Cataract Glasses?

Is bilberry a wonder supplement for your macular degeneration?
The jury is still out on that question. There is some supportive experimental data in animal models but no well-done human studies that show significant benefit.
What you shouldn’t do is pass up taking the AREDS 2 nutritional supplement formula, which is clinically proven to reduce the risk of severe visual loss that can happen with macular degeneration. Almost all the data supporting the POSSIBLE benefits of bilberry in visual conditions is related to NON-HUMANS. Stick with the AREDS 2 formula that has excellent clinical evidence.
So, what is bilberry and why do some people use it?
Bilberry (Vaccinium myrtillus), a low-growing shrub that produces a blue-colored berry, is native to Northern Europe and grows in North America and Asia. It is naturally rich in anthocyanins, which have anti-oxidant properties.
It is said that during World War II, British pilots in the Royal Air Force ate bilberry jam, hoping to improve their night vision. No one is exactly sure where the impetus to do this came from, but it is believed that this story is what lead to some widespread claims that bilberry was good for your eyes.
A study by JH Kramer, Anthocyanosides of Vaccinium myrtillus (Bilberry) for Night Vision - A Systematic Review of Placebo-Controlled Trials, reviewed most of the literature pertaining to the claim that bilberry improves night vision. He found that the four trials, which were all rigorous randomized controlled trials (RCTs), showed no correlation with bilberry extract and improved night vision. A fifth RCT and seven non-randomized controlled trials reported positive effects on outcome measures relevant to night vision, but these studies had less-rigorous methodology.
Healthy subjects with normal or above-average eyesight were tested in 11 of the 12 trials. The hypothesis that V. myrtillus improves normal night vision is not supported by evidence from rigorous clinical studies. There is a complete absence of rigorous research into the effects of the extract on subjects suffering impaired night vision due to pathological eye conditions.
Even though there is no solid evidence in human studies that bilberry produces any positive visual effects on night vision there is some experimental evidence that implies it might be useful in some ocular conditions whose mode of action is oxidative stress. There are recent epidemiologic, molecular and genetic studies that show a major role of oxidative stress in age-related macular degeneration.
There have been some studies showing oxidative protective effects of bilberry in non-human models.
In Protective Effects of Bilberry and Lingonberry Extracts Against Blue-light Emitting Diode Light-induced Retinal Photoreceptor Cell Damage in Vitro, Ogawa et al showed that cultured mouse cells that had bilberry extract added before subjection to high-energy short-wavelength light survived better than those that hadn't received the extract.
In Retinoprotective Effects of Bilberry Anthocyanins via Antioxidant, Anti-Inflammatory, and Anti-Apoptotic Mechanisms in a Visible Light-Induced Retinal Degeneration Model in Pigmented Rabbits, Wang et al found similarly improved survival of pigmented rabbit retinal cells when exposed to bilberry abstract prior to high-intensity light.
But bilberry is not without potential side effects.
Bilberry possesses anti-platelet activity and it might interact with NSAIDs, particularly aspirin. Excessive drinking of bilberry juice might cause diarrhea. One study of 2,295 people given bilberry extract found a 4% incidence of side effects or adverse events. Further, bilberry side effects may include mild digestive distress, skin rashes and drowsiness. Chronic uses of the bilberry leaf may lead to serious side effects. High doses of bilberry leaf can be poisonous.
Bilberry has not been evaluated by the Food and Drug Administration for safety, effectiveness, or purity.
Article contributed by Dr. Brian Wnorowski, M.D.
One of the hardest questions eye care professionals routinely have to deal with is when to tell people with visual difficulaties that they need to stop driving.
Giving up your driving privilege is difficult to come to terms with if you have a problem that leads to permanent visual decline.
The legal requirements for visual acuity vary from state to state. For example, in New Jersey the legal requirement to drive, based on vision, has been 20/50 vision or better with best correction in one eye for a “pleasure” driving license. For a commercial driving license, the requirement is 20/40 vision or better in both eyes.
In some states there is also a requirement for a certain degree of visual field (the ability to see off to the sides).
According to the Insurance Institute for Highway Safety, the highest rate of motor vehicle deaths per mile driven is in the age group of 75 and older (yes, even higher than teenagers). Much of this increased rate could be attributable to declining vision. There are also other contributing factors, such as slower reaction times and increased fragility, but the fact remains that the fatality rate is higher. , And so, when vision problems begin to occur with aging it is extremely important to do what is necessary to try to keep your vision as good as possible.
That means getting regular eye exams, keeping your glasses up-to-date, dealing with cataracts when appropriate, and staying on top of other vision-threatening conditions such as macular degeneration, glaucoma, and diabetes.
It is our responsibility to inform you when you are no longer passing the legal requirement to drive. Although not all states have mandatory reporting laws, your eye doctor will record in your medical record that you were informed that your vision did not pass the state requirements to maintain your privilege. And, yes, it is a privilege -- not a right -- to drive.
If you have a significant visual problem and your vision is beginning to decline, you need to have a frank discussion with your eye doctor about your driving capability. If you are getting close to failing the requirement, you need to start preparing with family and loved ones about how you are going to deal with not being able to drive.
Many of us eye doctors have had the unfortunate occurrence of having instructed a patient to stop driving because of failing vision, only to have him ignore that advice and get in an accident. Don’t be that person. Be prepared, have a plan.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

We have all heard the term ”Love is in the Air,” but can love really be in the eyes? Actually, Science has proven it so. Certain chemicals (or endorphins) that produce the emotion of love can be emitted through emotions expressed in the eyes. There are physiological changes in the eyes that occur when love is expressed between two individuals. Love for a romantic partner, a family member, or a favorite pet can all cause the same physical response: the pupil (black part in the center of the eye) dilates.
The size of the pupil can be an indication of emotional responses and messages. According to Scientific American, the autonomic nervous system (ANS), which directs our fight or flight response, causes the pupil to have a quick dilating response. The ANS is also in charge of heart rate and perspiration, and when a person is extremely interested in another person, the pupil has a dilating effect that is slightly less than the pupillary light reflex. This bounce in size is an automated response that gives scientists indication of mood or interest (or love) shown to a person or pet.
Mounting scientific evidence also shows the benefit of looking into the eyes of your pet, especially dogs. Stroking them causes you to become more healthy on all fronts, and a few minutes a day of lovingly looking at the dog and stroking the pet releases serotonin, prolactin, and oxytocin, which are "feel good" hormones.
There are also studies inspired by psychologist Arthur Aron, from over 20 years ago, that show if you stare into someone's eyes for 4 minutes you can fall in love... looking eye to eye allows you to connect with someone new or reminds you why you fell in love with this person in the first place.
Overall health is improved and years can be added to your life when looking at something or someone with love. Your eyes and autonomic nervous system play an intricate role in the expression of love.
Source:
12/07/2012 article of Scientific American entitled:
Why Do Pupils Dilate in Response to Emotional States?
By Joss Fong
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
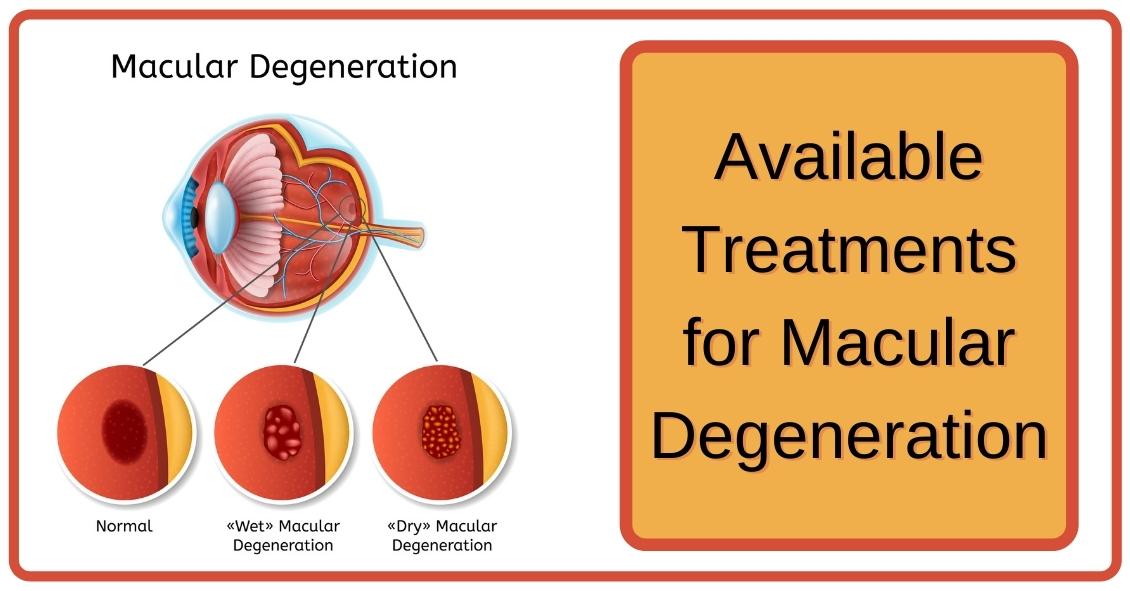
When confronted with a diagnosis of Age Related Macular Degeneration (AMD), it's natural to wonder what you should do. Here are some treatment options for both Dry and Wet Age Related Macular Degeneration.
Dry AMD Treatments
Nutrition Supplements
The Age-Related Eye Disease Study 2 (AREDS2) showed that people at high risk of developing advanced stages of AMD benefited from taking dietary supplements. Supplements lowered the risk of macular degeneration progression by 25 percent. These supplements did not benefit people with early AMD or people without AMD.
Following is the supplementation:
- Vitamin C - 500 mg
- Vitamin E - 400 IU
- Lutein – 10 mg
- Zeaxanthin – 2 mg
- Zinc Oxide – 80 mg
- Copper – 2 mg (to prevent copper deficiency that may be associated with taking high amount of zinc)
Another study showed a benefit in eating dark leafy greens and yellow, orange and other fruits and vegetables. These vitamins and minerals listed above are recommended in addition to a healthy, balanced diet.
It is important to remember that vitamin supplements are not a cure for AMD, nor will they restore vision. However, these supplements may help some people maintain their vision or slow the progression of the disease.
Wet AMD Treatments
Injection of Anti-VEGF
The most common treatment for wet AMD is an eye injection of anti-vascular endothelial growth factor (anti-VEGF). This treatment blocks the growth of abnormal blood vessels, slows their leakage of fluid, potentially helps slow vision loss, and in some cases, improves vision. There are multiple anti-VEGF drugs available: Avastin, Lucentis, and Eylea.
You may need monthly injections for a prolonged period of time for treatment of wet AMD.
Laser Treatment for Wet AMD
Some cases of wet AMD may benefit from thermal laser. This laser destroys the abnormal blood vessels in the eye to prevent leakage and bleeding in the retina. A scar forms where the laser is applied and may cause a blind spot that might be noticeable in your field of vision.
Photodynamic Therapy or PDT
Some patients with wet AMD might benefit from photodynamic therapy (PDT). A medication called Visudyne is injected into your arm and the drug is activated as it passes through the retina by shining a low-energy laser beam into your eye. Once the drug is activated by the light it produces a chemical reaction that destroys abnormal blood vessels in the retina. Sometimes a combination of laser treatments and injections of anti-VEGF mediations are employed to treat wet AMD.
Article contributed by Jane Pan M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
There have been studies undertaken over the past several years to try and understand if there are any of our day-to-day activities that either help or hurt the management of glaucoma.
Most of the studies demonstrated very little impact on the course of glaucoma. Here are some of the things researches have looked at.
Aerobic exercise: This means doing something at least four times per week for more than 20 minutes at a time that raises your pulse rate to a level that makes your heart work harder. Going from a sedentary lifestyle to active one with aerobic exercise resulted in a very slight decrease in baseline eye pressure.
Yoga: A study conducted at the Mount Sinai Health System (https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0144505) showed a significant increase in eye pressure with any head-down positioning. People with glaucoma would be wise to avoid any exercise that involves a position where your head is lower than your heart.
Weight lifting: Holding your breath while exerting yourself (called the Valsalva maneuver), is also a time when your eye pressure can go sky high. So if you lift weights for exercise, which is generally a good idea to maintain bone density, make it low weights with more repetitions of lifting, rather than heavy weights that make you grunt.
Wind instruments: A similar breath-holding problem applies to those playing the larger wind musical instruments like the French horn. One study suggested that there was a greater chance of glaucoma in symphonic wind players. If you play a brass instrument, it makes sense to have frequent checks of pressure, optic nerve head, and visual field.
Marijuana: Smoking marijuana can lower eye pressure. However, due to its short duration of action (3-4 hours), side effects, and lack of evidence that it alters the course of glaucoma, it is not recommended for glaucoma treatment.
Wearing tight neckties: This creates a very short-duration increase in eye pressure but doesn’t seem to have any long-term effects.

Ocular allergies are among the most common eye conditions to hit people of all ages.
Though typically worse in the seasons of Spring and Summer, some people suffer with allergies all year. This is especially true for people who have allergies to pet dander, mold, dust mites, and other common allergens that tend to linger throughout the year.
The hallmark sign of ocular allergies is itching.
While itching can be a symptom of other eye conditions, the likelihood that there is at least some allergy component to the condition is quite high. This seems to be particularly true when the itching occurs mainly in the inner corner of the eyes. This signals that the condition is allergy-related, whereas itching along the eyelid margin suggests other conditions.
Allergy itching is usually accompanied by redness, tearing, and string-like mucus discharge from the eye. When accompanied by rhinitis, sinusitis, and sneezing, people can truly suffer from their allergies - especially as it relates to the eye.
The good news is there are numerous avenues for relief from this annoying condition.
There are many over-the-counter antihistamine drops. Talk to your eye doctor about which ones are recommended.
In particularly severe cases, prescription antihistamine/mast cell stabilizer combination drops, or even topical steroids, can be used. In addition, cold compresses can be a great therapy in combination with the drops.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Living an overall healthy life is good for your eyes. Healthy vision starts with healthy eating and exercise habits.
There's more to complete eye health than just carrots. Are you eating food that promotes the best vision possible? Learn what foods boost your eye well-being and help protect against diseases. Here are important nutrients to look for when selecting your foods.
- Beta carotene or Vitamin A (helps the retina function smoothly): carrots and apricots
- Vitamin C (reduce risk of macular degeneration and cataracts): citrus and blueberries
- Vitamin E (hinders progression of cataracts and AMD): almonds and sunflower seeds
- Riboflavin (helps your eyes adapt in changes in light): broccoli and bell peppers
- Lutein (antioxidant to maintain health while aging): spinach and avacado
- Zinc (transfers vitamin A to the retina for eye-protective melanin productions and helps with night vision): beans and soy beans
- DHA (helps prevent Dry Eye): Fatty fish like salmon and tuna
Keep in mind, cooked food devalues the precious live enzymes, so some of these foods are best eaten raw.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.