

Dry eye is a very common problem that affects women more than men and becomes more prevalent as people get older.
It can present in many ways, with symptoms that can include a foreign body sensation, burning, stinging, redness, blurred vision, and dryness. Tearing is another symptom and occurs because the eye initially becomes irritated from the lack of moisture and then there is a sudden flood of tears in response to the irritation.
Unfortunately, this flood of tears can wash out other important components of the tear film that are necessary for proper eye lubrication. Signs and symptoms can range from mild to severe.
There are medications that have the potential to worsen the symptoms of dry eye. Here are some of the broad categories and specific medications that have been known to potentially worsen the symptoms:
- Blood Pressure Medications - Beta blockers such as Atenolol (Tenormin), and diuretics such as Hydrochlorothiazide.
- GERD (gastro-esophageal reflux disorder) Medications - There have been reports of an increase in dry eye symptoms by patients on these medications, which include Cimetidine (Tagamet), Rantidine (Zantac), Omerprazole (Prilosec), Lansoprazole (Prevacid), and Esomeprazole (Nexium).
- Antihistamines - More likely to cause dry eye: Diphenhydramine (Benadryl), loratadine (Claritin). Less likely to cause dry eye: Cetirizine (Zyrtec), Desloratadine (Clarinex) and Fexofenadine (Allegra). Many over-the-counter decongestants and cold remedies also contain antihistamines and can cause dry eye.
- Antidepressants - Almost all of the antidepressants, antipsychotic, and anti-anxiety drugs have the propensity to worsen dry eye symptoms.
- Acne medication - Oral Isotretinoin.
- Hormone Replacement Therapy - The estrogen in HRT has been implicated in dry eye.
- Parkinson's Medication - Levodopa/Carbidopa (Synamet), Benztropine (Cogentin), Procyclidine (Kemadrin).
- Eye Drops - In addition to oral medications many eye drops can actually increase the symptoms of dry eye, especially drops with the preservative BAK.
If you are suffering from dry eye and are using any of the medications above you should discuss this with your eye doctor and medical doctor. Don't stop these medications on your own without consulting your doctors.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

We are frequently asked if it’s wise to have cataract surgery if you have Macular Degeneration.
Let’s start with some background.
- Cataracts and Age-related Macular Degeneration (AMD) are both leading causes of visual impairment in the elderly population.
- Cataracts develop when the normal clear lens gets cloudy with age. This is correctable with cataract surgery, which involves replacing the cloudy lens with a clear, artificial lens.
- While cataracts affect the front part of the eye, AMD causes damage to the retina, which is the inner back lining of the eye.
In the past, there was a concern about cataract surgery causing progression of AMD. It was thought that there was an inflammatory component to AMD and the normal inflammatory response after cataract surgery may lead to AMD progression.
But studies have looked at patients who underwent cataract surgery compared to patients who didn't have cataract surgery and the progression of AMD was not significantly different between the two groups. However, those patients with AMD who underwent cataract surgery had a significant improvement in vision.
AMD patients can further be characterized as having wet or dry AMD, and only those with wet AMD require treatment. Patients with wet AMD need injections to decrease the growth of new blood vessels and reduce fluid in the retina.
A 2015 study showed that after cataract surgery, there was an increase in fluid in the retina of patients with wet AMD. Therefore, in patients with wet AMD, we usually want the wet AMD to be stabilized before the patient has cataract surgery. Sometimes an injection may be given prior to cataract surgery to prevent any inflammatory changes that may be associated with cataract surgery.
The majority of the studies on the subject conclude that it is safe to have cataract surgery even if you have AMD and in most cases there is a significant improvement in vision. Removing the cloudy lens also helps the ophthalmologist to better monitor the status of the AMD.
Article contributed by Dr. Jan Pan.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Read more: What About Cataract Surgery with My Macular Degeneration?
It's pretty common for eye doctors to have older patients come in asking if the white part of their eye, the sclera, has a growth or is turning a gray color.
Usually, the culprit is senile scleral plaque, which is commonly seen in people over the age of 70. It is a benign condition and more commonly seen in women. This condition is symmetrically found on both sides of the eye and is due to age-related degeneration and calcification of the eye muscle insertion into the eye. In one study, the size of the senile scleral plaque increased as the person aged and was not associated with any medical conditions. People are asymptomatic, as the plaques do not affect vision and no treatment is needed.
Another commonly asked question is: Why is the colored part of my eye turning white?
The colored part of the eye is the iris, which is covered by a clear layer called the cornea. It is actually the edge of the cornea that attaches to the white part of the eye that becomes grey or whitish colored.
This condition is called arcus senilis, which is seen in over 60% of people over the age of 60 and approximately 100% over the age of 80. There is no visual impairment and no treatment is needed. Sometimes when this condition is seen in younger patients, it may be related to high cholesterol, so a visit to the primary care doctor may be needed.
These are two very commonly encountered conditions that may cause distress for patients because it seems like their eyes are changing colors.
Thankfully, no treatment is needed for these two conditions, as they do not affect vision.
Article contributed by Dr. Jane Pan
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Recent Census Bureau data shows a population of approximately 71 million baby boomers (the generation born from 1946-1964). What does that have to do with low vision you may ask? Approximately 40 million people worldwide have some sort of blindness, and aging increases the incidence of macular degeneration and other vision impairment that qualifies them as “low vision” persons.
Low vision is a condition of the eye in which the vision falls below 20/70 in the better seeing eye. It impairs the recipients, rendering them unable to perform daily tasks that others take for granted. With this rising aging population, the awareness of low vision therapy, diagnosis, and treatments are more widely available.
Low vision treatment can help people recover from decreased visual function due to retinal disease, brain injury, neurological damage, and other causes.
It is not only the elderly population that is affected--approximately 20% of low vision patients are children under the age of 18. Childhood genetic disorders of the eye such as retinitis pigmentosa, albinism, Bests disease, ROP, rod/cone disorders, and glaucoma are among the causes of low vision in the pediatric population.
What can be done to help these millions?
There are eye care practitioners that specialize in low vision, as well as therapists. They train the patient to adjust their current lifestyles to make them more independent and utilize the current salvageable vision they do have. For example, if a person has lost their central vision due to macular degeneration, they can be trained to use their peripheral vision to accommodate for many tasks.
Because patients with low vision cannot be corrected with regular eye glasses, the use of telescopes, magnifiers, computer generated aids, training, biofeedback, and optical magnification devices are among some of the resources available to help. Occupational therapists also employ orientation and mobility assistance to help patients in their daily living skills.
There are many technologies that help to improve vision. One such technology is a bionic eye device that uses a pair of glasses with a camera that transmits video data to an implant in the back of that patients eye (the retina). This device uses technology similar to cochlear implants that stimulate auditory nerve signals to restore hearing. In the same way, visual impulses can be restored by stimulating neurons in the retina, brain, or optic nerve.
Maybe the Bionic Man TV series wasn’t too far out there and can someday be a reality............restoring vision to millions.
For more valuable information on low vision visit:
American Optometric Association AOA
American Occupational Therapy Association AOTA
American Academy of Ophthalmology AAO
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Age-related macular degeneration, often called ARMD or AMD, is the leading cause of vision loss among Americans 65 and older.
AMD causes damage to the macula, which is the central portion of the retina responsible for sharp central vision. AMD doesn't lead to complete blindness because peripheral vision is still intact, but the loss of central vision can interfere with simple everyday activities such as reading and driving, and it can be very debilitating.
Types of Macular Degeneration
There are two types of macular degeneration: Dry AMD and Wet AMD.
Dry (non-exudative) macular degeneration constitutes approximately 85-90% of all cases of AMD. Dry AMD results from thinning of the macula or the deposition of yellow pigment known as drusen in the macula. There may be gradual loss of central vision with dry AMD, but it is usually not as severe as wet AMD vision loss. However, dry AMD can slowly progress to late-stage geographic atrophy, which can cause severe vision loss.
Wet (exudative) macular degeneration makes up the remaining 10-15% of cases. Exudative or neovascular refers to the growth of new blood vessels in the macula, where they are not normally present. The wet form usually leads to more serious vision loss than the dry form.
AMD Risk factors
- Age is the biggest risk factor. Risk increases with age.
- Smoking. Research shows that smoking increases your risk.
- Family history. People with a family history of AMD are at higher risk.
- Race. AMD is more common in Caucasians than other races, but it exists in every ethnicity.
- Gender. AMD is more common in women than men.
Detection of AMD
There are several tests that are used to detect AMD.
A dilated eye exam can detect AMD. Once the eyes are dilated, the macula can be viewed by the ophthalmologist or optometrist. The presence of drusen and pigmentary changes can then be detected.
An Amsler Grid test uses pattern of straight lines that resemble a checkerboard. It can be used to monitor changes in vision. The onset of AMD can cause the lines on the grid to disappear or appear wavy and distorted.
Fluorescein Angiogram is a test performed in the office. A fluorescent dye is injected into the arm and then a series of pictures are taken as the dye passes through the circulatory system in the back of the eye.
Optical coherence tomography (OCT) is a test based on ultrasound. It is a painless study where high-resolution pictures are taken of the retina.
Article contributed by Jane Pan M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

At some point, you might be the victim of one of these scenarios: You rub your eye really hard, you walk into something, or you just wake up with a red, painful, swollen eye. However it happened, your eye is red, you’re possibly in pain, and you’re worried.
What do you do next?
Going to the Emergency Room is probably not your best bet.
Your first reaction should be to go see the eye doctor.
There are many causes for a red eye, especially a non-painful red eye. Most are relatively benign and may resolve on their own, even without treatment.
Case in point: Everyone fears the dreaded “pink eye,” which is really just a colloquial term for conjunctivitis, an inflammation or infection of the clear translucent layer (conjunctiva) overlying the white part (sclera) of our eye. Most cases are viral, which is kind of like having a cold in your eye (and we all know there is no cure for the common cold).
Going to the ER likely means you’re going to be prescribed antibiotic drops, which DO NOT treat viral eye infections. Your eye doctor may be able to differentiate if the conjunctivitis is viral or bacterial and you can be treated accordingly.
Another problem with going to the ER for your eye problem is that some Emergency Rooms are not equipped with the same instruments that your eye doctor’s office has, or the ER docs may not be well versed in utilizing the equipment they do have.
The primary instrument that your eye doctor uses to examine your eye is called a slit lamp and the best way to diagnose your red eye is a thorough examination with a slit lamp.
Some eye conditions that cause red eyes require steroid drops for treatment. NO ONE should be prescribing steroids without looking at the eye under a slit lamp. If given a steroid for certain eye conditions that may cause a red eye (such as a Herpes infection), the problem can be made much worse.
Bottom line: If you have an eye problem, see an eye doctor.
Going to the ER with an eye problem can result in long periods of waiting time. Remember, you are there along with people having heart attacks, strokes, bad motor vehicle accidents and the like-- “my eye is red” is not likely to get high priority.
Whenever you have a sudden problem with your eye your first move should be to pick up the phone and call an eye doctor. Most eye doctor offices have an emergency phone number in case these problems arise, and again, if there is no pain or vision loss associated with the red eye, it is likely not an emergency.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
A quick explanation and background of a progressive addition lens (or PAL) is necessary in order to understand the importance of choosing the proper lens for your needs.
A progressive lens gives people an array of prescriptions - placed in the proper positions throughout the lens - to best imitate normal vision. Imagine having the precise correction needed to see a television screen more than 15 feet from you, while reading this article on your desktop computer, and then looking down at your keyboard in order to start entering the address to your favorite website. This, in a nutshell, is exactly what the progressive lens is ideally capable of accomplishing with one pair of glasses.
Having the least amount of peripheral distortion, and one of the wider ranges in both distance power, astigmatism, prism, and add power availability, we find this lens to be very versatile. The most important thing to you is that this product feels very natural in front of your eye. For first-time progressive lens wearers, there is a stigma that it takes a bit of time to adjust to a lens that holds multiple prescriptions. This is often still an issue if places use old technology lenses or don’t take careful measurements to assure the proper placement on the lens in the frame. However, with modern technology, the use of computers to fine tune this amazing product, and careful measurements and lens positioning by your optician, this lens does the best job we have seen in mimicking perfect 20/20 vision at all focal lengths.
Along with the progressive lens itself, there are other additional treatments, or “add-ons” that can immensely improve one’s experience with their glasses. These options include photochromic lenses, anti-reflective coatings, and polycarbonate scratch-resistant lenses. Talk with your eyecare team about what options might work best for you!
Article contributed by Richard Striffolino Jr.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
The word “astigmatism” is used so much in the optometric world that most people have talked about it when discussing their eye health with their doctor.
“Astigmatism” comes from the Greek “a” - meaning “without” - and “stigma” - meaning “a point.” In technical ocular terms, astigmatism means that instead of there being one point of focus in the eye, there are two. In other words, light merges not on to a singular point, but on two different points.
This is experienced in the real world by blurred, hazy vision, and can sometimes lead to eye strain or headaches if not corrected with either glasses or contact lenses.
Astigmatism is not a disease. In fact, more than 90% of people have some degree of astigmatism.
Astigmatism occurs when the cornea, the clear front surface of the eye like a watch crystal, is not perfectly round. The real-world example we often use to explain astigmatism is the difference between a basketball and a football.
If you cut a basketball in half you get a nice round half of a sphere. That is the shape of a cornea without astigmatism.
If you cut a football in half lengthwise you are left with a curved surface that is not perfectly round. It has a steeper curvature on one side and a flatter curve on the other side. This is an exaggerated example of what a cornea with astigmatism looks like.
The degree of astigmatism and the angle at which it occurs is very different from one person to the next. Therefore, two eyeglass prescriptions are rarely the same because there are an infinite number of shapes the eye can take.
Most astigmatism is “regular astigmatism,” where the two different curvatures to the eye lie 90 degrees apart from one another. Some eye diseases or surgeries of the eye can induce “irregular astigmatism,” where the curvatures are in several different places on the eye’s surface, and often the curvatures are vastly different, leading to a high amount of astigmatism.
Regular astigmatism is treated with glasses, contact lenses, or refractive surgery (PRK or LASIK). Irregular astigmatism, such as that caused by the eye disease keratoconus, usually cannot be treated with these conventional methods. In these circumstances, special contact lenses are needed to treat the condition.
The next time you hear that either you or a loved one has astigmatism, fear not.
It is easily corrected, and although astigmatism can cause your vision to be blurry, it rarely causes any permanent damage to the health of your eyes.
If you experience blurred vision, headaches, or eye strain, having a complete eye exam may lead to a diagnosis and treatment of this easily-dealt-with condition.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Read more: Why Having Astigmatism Isn't Usually That Big a Deal
There are several different variations of glaucoma, but in this article we will mainly focus on Primary Open Angle Glaucoma. This means that there is no specific underlying cause for the glaucoma, like inflammation, trauma or a severe cataract. It also means that the drainage angle where fluid is drained from the inside of the eye into the bloodstream is not narrow or closed.
Closed or Narrow Angle Glaucoma, which we won't be discussing today, is treated differently from Open Angle Glaucoma
In the U.S., Primary Open Angle Glaucoma (POAG) is by far the most common type of glaucoma we treat.
Glaucoma is a disease where the optic nerve in the back of the eye deteriorates over time, and that deterioration has a relationship to the Intraocular Pressure (IOP). Most - but not all - people diagnosed with glaucoma have an elevated IOP. Some people have fairly normal IOP’s but show the characteristic deterioration in the optic nerve. Regardless of whether or not the pressure was high initially, our primary treatment is to lower the IOP. We usually are looking to try to get the IOP down by about 25% from the pre-treatment levels.
The two mainstays of initial treatment for POAG in the U.S. are medications or laser treatments. There are other places in the world where glaucoma is initially treated with surgery. However, while surgery can often lower the pressure to a greater degree than either medications or laser treatments, it comes with a higher rate of complications. Most U.S. eye doctors elect to go with the more conservative approach and utilize either medications, most often in the form of eye drops, or a laser treatment.
Drops
There are several different classes of medications used to treat glaucoma.
The most common class used are the Prostaglandin Analogues or PGA’s. Some of the PGA’s available in the U.S. are Xalatan (latanaprost), Travatan (travapost), Lumigan (bimatoprost) and Zioptan (tafluprost).
PGA’s are most doctors’ first line of treatment because they generally lower the IOP better than the other classes, they are reasonably well tolerated by most people, and they are dosed just once a day, while most of the other drugs available have to be used multiple times a day.
The other classes of drugs include beta-blockers that are used once or twice a day; carbonic anhydrase inhibitors (CAI’s ), which come in either a drop or pill form and are used either twice or three times a day; alpha agonists that are used either twice or three times a day; and miotics, which are used three or four times a day. All of these other medications are typically used as either second-line or adjunctive treatment when the PGA’s are not successful in keeping the pressure down as single agents.
There are also several combination drops available in the U.S. that combine two of the second-line agents (Cosopt, Combigan, and Symbrinza).
Laser
The second option for initial treatment is a laser procedure.
Two common laser treatments for Open Angle Glaucoma are Argon Laser Trabeculoplasty (ALT) or Selective Laser Trabeculoplasty (SLT). These treatments try to get an area inside the eye called the trabecular meshwork - where fluid is drained from the inside of the eye into the venous system - to drain more efficiently.
These treatments tend to lower the pressure to about the same degree as the PGA’s do with over 80% of patients achieving a significant decrease in their eye pressure that lasts at least a year. Both laser treatments can be repeated if the pressure begins to rise again in the future, but the SLT works slightly better as a repeat procedure compared to the ALT.
Article contributed by Dr. Brian Wnorowski, M.D.
Read more: Just Found Out I Have Primary Open Angle Glaucoma. What Now?

There is an old adage in the eye care industry--Glasses are a necessity, contact lenses are a luxury. Ninety-nine percent of the time this is absolutely true. In the absence of unusual eye disorders or very high prescriptions that don’t allow a person to wear glasses comfortably, contact lenses should only ever be worn if there is a good, sturdy, updated set of prescription glasses available, too. This is due to the fact that there are often emergencies where people cannot wear their contact lenses.
In the 21st century, contact lens technology has gotten to the point where we have drastically cut down on the number of adverse events related to contact lens wear. However, human beings were not meant to wear little pieces of plastic in their eyes. Contact lenses are still considered a foreign body in the eye, and sometimes with foreign bodies, our eyes might feel the need to fight back against the “invader.” As such, issues like red eyes, corneal ulcers, eyelid inflammation, dry eyes, and abnormal blood vessel growth can result from wearing contact lenses.
More often than I would like, I have patients who are longtime contact lens wearers come in, and when I inquire as to the condition of their glasses, they say they don’t own any. My next question is inevitably, “What happens if you get an eye infection and you can’t wear your contacts?” I then see the proverbial light bulb go off in their heads followed by a blank stare. Why? “Because I’ve never had a problem before.” Well, just because you maybe have never been in a car accident before, doesn’t mean you shouldn’t wear your seat belt!
I will therefore repeat the most important takeaway here--Glasses are a necessity, contacts are a luxury. Even if you don’t want to go “all out” and get the most expensive frames or lenses in your glasses, having a reliable pair of glasses is an absolute must for any contact lens wearer.
Article contributed by Dr. Jonathan Gerard
In light of the holiday season, here are our top 10 eye care jokes.
1) What do you call a blind deer? No Eye Deer!
2) What do you call a blind deer with no legs? Still No Eye Deer!
3) Why do eye doctors live long lives? Because they dilate!
4) Why did the blind man fall into the well? He couldn’t see that well.
5) Why shouldn’t you put avocados on your eyes? Because you might get guac-coma!
6) What did the right eye say to the left eye? "Between you and me, something smells."
7) A man goes to his eye doctor and tells the receptionist he’s seeing spots. The receptionist asks if he’s ever seen a doctor. The man replies, “No, just spots.”
8) How many eye doctors does it take to screw in a light bulb? One … or two
9) Unbeknownst to her, a woman was kicked out of peripheral vision club. She didn’t see that one coming!
10) What do you call a blind dinosaur? A do-you-think-he-saurus
Bonus: What do you call a blind dinosaur’s dog? A do-you-think-he-saurus rex!
Article contributed by Dr. Jonathan Gerard
Red, Itchy, swollen eyelids are often due to a condition called blepharitis. Blepharitis tends to be a chronic condition due to thick eyelid mucous gland production that sticks to the bases of the eyelashes. This adherent mucous can allow bacteria to overgrow and also attract and retain allergens. The standard treatment for blepharitis is doing warm compresses and cleaning off the eyelids with a mild baby shampoo and water solution. This treatment works for some people but there are many more sufferers who have chronic irritation and relapses despite this treatment. If the warm compresses and eyelid scrubs are not quite keeping the condition under control there are several other additional treatments that can be used to control the symptoms. One such treatment that your doctor may decide upon is to use an antibiotic/steroid combination drop or ointment. We usually use these for short periods of time to try to bring the condition under control. They are not good to use chronically because it can build resistant bacteria and the steroid component can cause other eye issues like cataracts and glaucoma. The treatment is very safe for short term use but chronic use is usually not a good option. There are also antibiotic eyelid scrubs such as Avenova which can be prescribed and used on a more long-term basis. Oral Doxycycline can also be used longer in very low doses. Doxycycline is an antibiotic that when used to treat infections is generally prescribed in a dose of 100mg twice a day. For chronic Blepharitis suffers we generally use a much lower dose of around 50 mg a day. At that dose we are using the Doxycycline to help thin out the mucous production from the eyelid glands more than for its antibiotic properties. In summary, blepharitis can be a chronic issue that requires some persistent “maintenance” work be done to keep it under control, with further intervention sometimes needed for flare-ups.
Article contributed by Dr. Brian Wnorowski, M.D.
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ
Choroidal nevus is the fancy term for a freckle in the back of the eye.
This lesion arises from a collection of cells that make pigment in the choroid, which lines the back of the retina and supplies the retina with nutrients. These choroidal nevi (plural of nevus) are usually grayish in color and develop in about 5-10% of the adult population. They are usually asymptomatic and detected during a routine dilated eye exam.
Just like any freckle on our body, we should monitor it for any change in size or growth. This is usually done with a photograph of the nevus and annual exams are normally recommended to monitor any change.
In addition to a photograph, other tests that can be used to monitor the nevus are:
- Optical coherence tomography - a test that uses light waves to take cross-section pictures of the retina. This test is used to detect if the nevus is elevated or if fluid is present underneath the retina.
- Ultrasound - uses sound waves to measure the size and elevation of the nevus.
- Fluorescein angiography - a dye test to detect abnormal blood flow through the nevus.
The concern is for transformation of the choroidal nevus into melanoma, a cancer in the eye. It has been estimated that 6% of the population have choroidal nevus and 1 in 8,000 of these nevi transform into melanoma. Some factors predictive of possible transformation in melanoma are:
- Thickness of the lesion, greater than 2 mm.
- Subretinal fluid, observed on exam or optical coherence test.
- Symptoms that include decreased or blurry vision, flashes, or floaters.
- Orange pigment in the lesion.
- Located near the optic nerve.
Early detection of choroidal melanoma results in earlier treatment and better outcomes for the patient. Many times, a patient with choroidal melanoma may be asymptomatic, and so routine dilated eye exams should be performed to identify any suspicious choroidal nevus.
In general, there is no treatment for choroidal nevus other than observation and monitoring for change. Therefore, a visit to your eye doctor is recommended to detect any freckles in the back of your eye.
Article contributed by Dr. Jane Pan

A common in-office procedure is an eye injection for treatment of various eye conditions, such as wet macular degeneration, diabetic retinopathy, or vein occlusion.
It is normal to be anxious prior to your first eye injection but knowing what to expect may alleviate some anxiety.
Your eye will be numbed with topical anesthetic drops. Usually, a cotton-tipped applicator soaked in anesthetic will be held against the white part of the eye to numb it. Sometimes, a thick gel may also be used for numbing. Once the eye is numbed, it will then be cleaned and a small instrument will be used to hold the eye open. During the actual injection, some patients feel pressure while others may feel a quick sting. Each person will have a different experience and each injection will be different.
The medicine is injected into the white part of the eye. Sometimes a blood vessel may be encountered during the injection and you may notice a little redness on the outside of the eye. This is purely a cosmetic symptom and the redness will disappear within the next couple of days. Patients may also experience some mild irritation after the injection due to the drops that are placed in the eye. I usually recommend over-the-counter artificial tears to use after the injections. Usually, the eye should feel normal by the next day.
Another common symptom after an injection are floaters. These floaters usually appear as small bubbles in the lower half of your vision, but they will disappear in in a day or two.
There are no activity restrictions after the injection and no antibiotic drops are needed.
Things to watch for after the injection:
- If your eye gets painful or redness develops a couple of days after the injection, then you should call your doctor.
- If your vision declines or you notice increased or hundreds of floaters then you should call to be seen.
Otherwise, patients are usually initially seen once a month after they first start injections
Article contributed by Dr. Jane Pan
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

A common question asked during the eye exam is, “When is the puff coming?”
Patients are referring to air-puff or non-contact tonometry. Tonometry is the procedure used to measure eye pressure, and this is important for diagnosing and monitoring glaucoma.
In non-contact tonometry, a puff of air is used to measure the pressure inside the eye. The benefit of this test is there is no actual contact with the eye, but the air puff is sometimes very startling for patients. Most people hate that test and it isn’t the most accurate way to measure your eye pressure.
Some doctors don’t even use the air-puff test. Instead, they place a yellow drop that consists of a numbing medicine and then shine a blue light on the eye. This is done in front of the slit lamp and a small tip gently touches the eye to measure the eye pressure. This procedure is called Goldmann tonometry and is considered the gold standard for measuring eye pressure.
Another method for checking eye pressure is the Tonopen. This is a portable, hand-held instrument that is useful when patients can’t sit in front of the slit lamp to have their eye pressure checked. The Tonopen also requires a numbing drop to be placed in the eye, and the tip gently touches the eye.
A common question related to tonometry is “what normal eye pressure?”
Normal eye pressure ranges from 10-21 mm Hg. Eye pressure doesn't have any relationship to blood pressure. Many times, people are surprised that their eye pressure is high, but they have normal blood pressure. In general, there is no diet or exercise that will significantly affect eye pressure. It is therefore important to have your eye pressure checked regularly because there are usually no symptoms of high eye pressure until it has affected your vision.
Article contributed by Dr. Jane Pan
Read more: Why Do You Have to Touch My Eye or Puff It with Air?

Not everyone understands the importance of sunglasses when the weather turns cold.
Polarized sunglasses are usually associated with Summer, but in some ways it is even more important to wear protective glasses during the Winter.
It’s getting to be that time of year when the sun sits at a much different angle, and its rays impact our eyes and skin at a lower position. This translates to an increase in the exposure of harmful UV rays, especially if we are not wearing the proper sunglasses as protection.
Polarized sunglasses, which are much different than the older dye-tinted lenses, are both anti-reflective and UV resistant. A good-quality polarized sunglass lens will protect you from the entire UV spectrum. This not only preserves your vision, but it also protects the skin around the eyes, which is thought to have a much higher rate of susceptibility to skin cancer.
Snow poses another issue that can be countered by polarized sunglasses.
Snow on the ground tends to act as a mirror because of its white reflective surface and this reflection can become a hindrance while driving. The anti-reflective surface of polarized sunglasses helps reduce the glare and gives drivers improved visibility.
Polarized sunglasses come in many different options based on a patient’s needs. Whether it’s single-vision distance lenses, bifocals, or progressive lenses, there is a polarized lens for every patient.
Winter is a great time of year to ask your optical department about purchasing polarized sunglasses.
Article contributed by Richard Striffolino Jr.
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ
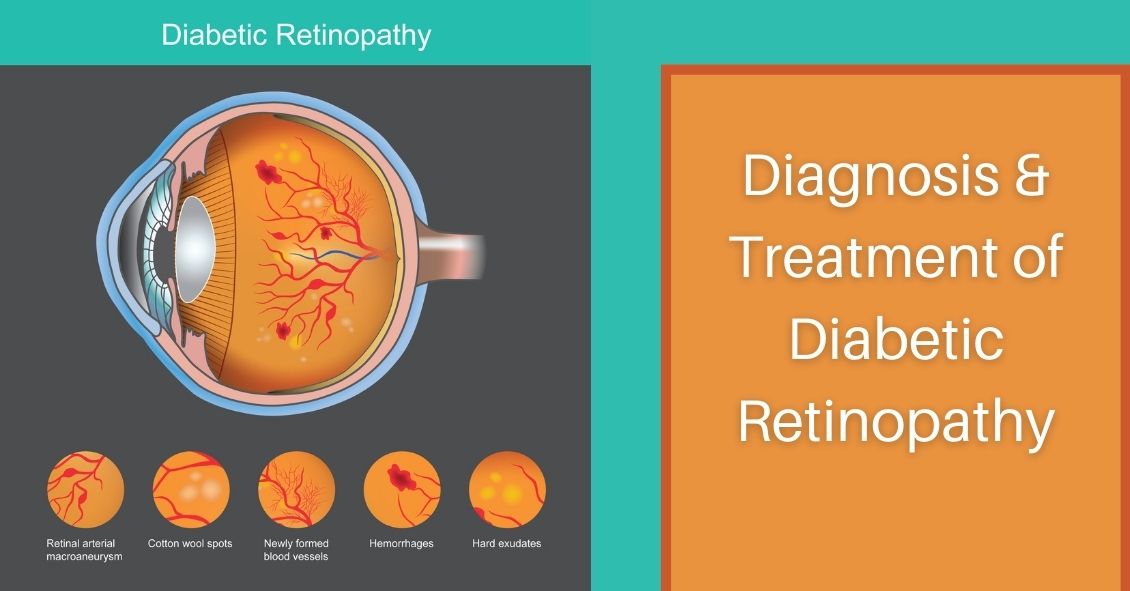
Diabetic retinopathy, which is a complication of diabetes that affects the eyes, is detected during a comprehensive eye exam that includes:
- Visual acuity testing.
- Dilated exam in which drops are placed to widen the pupil to allow examination of the retina.
- Tonometry. Measurement of the eye pressure inside the eye.
Supplemental testing may include:
- Optical coherence tomography (OCT). This is a non-invasive test that images the retina to detect any fluid or diabetic macular edema.
- Fluorescein Angiography. This test involves an injection of a dye into your arm and a series of pictures that are taken as the dye flows through the retinal vessels. This may show leakage of fluid or the growth of new blood vessels in the retina.
Treatment for Diabetic Retinopathy
The best treatment is prevention of diabetic retinopathy by strict control of blood sugars. Once diabetic retinopathy is present, treatment of diabetic retinopathy will slow progression but won’t cure it.
Diabetic macular edema can be treated with several different therapies that may be used alone or in combination.
These include:
- Injection therapy. Anti-VEGF drugs are injected into the eye to block a substance called vascular endothelial growth factor (VEGF). This medication will block abnormal blood vessel growth and decrease the leakage of fluid into the retina. The three most commonly used drugs include Avastin, Lucentis and Eylea. Steroids are another option for treatment of diabetic macular edema but are used less often due to side effects of possible cataracts and increased eye pressure.
- Laser therapy. Small laser burns are applied in the area of the retinal swelling to slow the leakage of fluid. Laser treatment can be combined with anti-VEGF injections.
Proliferative diabetic retinopathy can be treated with:
- Laser therapy. Laser is applied on the retina to shrink the new blood vessels and to prevent bleeding inside the eye. Bleeding inside the eye will cloud the vision and cause floaters, which are small moving spots that appear in your field of vision.
- Surgery. When there is significant amount of blood or scar tissue inside the eye, then a vitrectomy surgery is performed to remove the blood and scar tissue. Laser and anti-VEGF therapy may also be applied during the surgery.
In the end, the best treatment is prevention of diabetic retinopathy. An annual comprehensive dilated eye exam is recommended for anyone who has been diagnosed with diabetes, since early mild non-proliferative diabetic retinopathy can show no symptoms.
Article contributed by Jane Pan M.D.
The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ
Parkinson’s disease is a progressive degenerative condition of the neurological system. The majority of Parkinson’s effects are on movement, often starting off very slowly and subtly. One of the earliest symptoms is a slight tremor in one or both hands. Other early symptoms include a lack of facial expression and decreased blinking of the eyes, so it looks like the person is always staring.
The next stage usually results in difficulty with initiating movement, especially walking. It frequently looks like it takes a tremendous concentrated effort to initiate walking and the steps often start off very small with a shuffling of the feet. At the same time, the disease stiffens the muscles of the arms so that when the person is walking there is a noticeable decrease in the swinging of the arms. Speech becomes much softer and writing becomes more of an effort, with handwriting getting smaller and smaller as the disease progresses.
Parkinson’s can also affect your visual performance, mainly in two parts of your eyes: the tear film and the ocular muscles.
It affects your tear film because of the decreased rate of blinking. The tear film is an important component of your optical system. It coats the surface of the cornea and if it is not smooth and uniform the result is a blurring of your vision. Blinking helps refresh your tear film and spreads it out uniformly. It is analogous to the washers and wipers on your car. If the windshield (like your cornea) is spotty you have a hard time seeing through that windshield. Turn on the washers and now there is more moisture on the surface but that is also spotty and hard to see through until the wipers go by and spread the moisture out evenly. That is very similar to how your cornea, tear film and your eyelids blinking interact to keep your vision clear.
If you don’t blink enough, the tear film begins to dry out in spots and having dry spots next to moist spots results in an irregular film and therefore blurred vision. That is how the decreased blinking frequency in people with Parkinson’s disease results in a complaint of intermittent blurred vision.
The other way the disease affects your vision is by creating a problem called convergence insufficiency. When you read, your two eyes turn inward toward each other in a process called convergence. Your eye muscles are activated in order to have the two eyes point inward to focus on the near object. By interfering with the interaction between your nerves and muscles, Parkinson’s makes it difficult to both initiate and sustain the convergence you need to keep both eyes focused on a near object.
This sometimes results in a disconnect between what a person is capable of reading on an eye chart for a short period of time and what happens after trying to sustain the effort over a longer period of time. This disconnect can result in some frustration. Often during an exam, a quick look at the distance eye chart allows the patient to see fairly well because the dry eye may not be causing any blurring if the patient just blinked a few times before reading the chart. A patient may also do well on the near chart because they are often being tested one eye at a time. When you read things up close with just one eye there is no need for the eyes to converge so they do well one eye at a time.
There are some other less-frequent eye problems that can occur with Parkinson’s. One is called blepharospasm, where the eyelids on either one side or both forcefully close involuntarily. A person can also end up with a condition called apraxia of eye opening, where they can’t voluntarily open the eyelids. This is different from blepharospasm because in this condition the lids are not being forcefully closed, they just won’t open when you want them to.
The majority of these problems do improve if the Parkinson’s is treated with medication or even brain stimulation.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided on this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Shingles is the term we use to describe a condition that is caused by a re-activation of the Herpes Varicella-Zoster virus. The origin of this infection usually goes way back to childhood with a disease we know as chickenpox.
When you have a chickenpox infection your immune system manages to eventually suppress that virus from causing an active infection, but the virus does not get completely eliminated from your body--it is able to go and hide in your nerve roots.
Your immune system manages to keep the virus in check for most of your life but there may come a time in adulthood when your immune system is not working as well as it used to, and the virus can reappear. It usually does this along the distribution of a single sensory nerve called a dermatome.
The most common area for this to occur is along your trunk (chest or abdomen) but it is also commonly found on the face.
There are three branches of nerves that supply sensation to your face. They are all branches of the fifth cranial nerve. Those three branches supply the upper face (V1), the mid face (V2), and the lower face (V3). Most of the time, shingles breaks out along only one of the branches at a time. The one that most frequently involves the eye is a rash breakout in the V1 distribution. This can involve the forehead and both the upper and lower eyelid. It is also much more likely that the inside of the eye will be involved if the tip of the nose has a lesion on it. The reason for that is that there is a specific subbranch of the V1 nerve called the nasocilliary nerve. This nerve is responsible for sensation on the tip of the nose and the inside of the eye.
The hallmark of shingles is that once the rash erupts it stays on one side of the body, including when it happens on the face. The rash will go up to the centerline of your face but will not go to the other side. You may get lesions on your scalp, but they will not show up on the back of your head. That is because the V1 does not go past half way back on your scalp. The back of your head has its sensation handled by nerves that come out of your spinal cord not cranial nerves that come out of the front of your skull.
Many people have a hard-to-describe sensation of pain, irritation, or itching along the distribution of the nerve for a day or two before the rash shows up. It is important to recognize the rash as quickly as possible because the drugs that treat shingles--usually Acyclovir, Famvir (famciclovir), or Valtrex (valacyclovir)--are much more effective if they are started within three days of the beginning of the rash.
Eye problems may occur along with the rash, especially if there is a lesion on the tip of the nose.
The two biggest problems are swelling or inflammation of the cornea and inflammation inside the eye, which we call iritis or uveitis.
The inflammation in the eye can cause pain and it can also increase eye pressure and cause glaucoma. Most often the treatment for the eye problem is to use the same oral medication mentioned above and sometimes it also can require eye drops to decrease the inflammation the virus is causing (steroid drops) or drops to try and lower the elevated pressure (glaucoma drops).
The eye inflammation can cause blurred vision, pain, and significant light sensitivity. It can be hard to treat and control and can continue to be a problem long after the skin lesions are gone. In fact, many times problems don’t even start until the skin lesions are starting to go away.
It is recommended that if you have shingles affecting the distribution of V1 that you have an eye exam within a few days of the diagnosis being made and then again a week later because, as mentioned above, the eye problems can present a week later than the skin eruptions.
There can be some serious long-term effects of shingles on your eye, including glaucoma and corneal scarring that can be bad enough to require a corneal transplant. The symptoms are often obvious with the vision being blurry and the eye being very red and painful, but sometimes the symptoms may be much more mild even when significant trouble is brewing inside the eye. So even if you think the eye feels fine, you need an exam to ensure there is not subtle inflammation or significant elevation of the pressure in the eye.
The other long-term problem with shingles around the eye is the possibility of there being ongoing pain in the area that can last for many years. This is called Post Herpetic Neuralgia (PHN). This pain can occur all along the dermatome where shingles had occurred. The eye itself may look perfectly normal but the pain persists. This is often treated with drugs that were originally developed as seizure medication but have since been shown to help alleviate neurological pain. The two most commonly used drugs for this are Neurontin (Gabapentin) and Lyrica (Pregabalin).
The most important thing you can do to try and make sure this doesn’t happen to you is to be vaccinated for shingles. The original vaccination called Zostavax has been available since 2006 in the U.S. It is a single-injection vaccine and was recommend for everyone over 60. The main issue with this vaccine is that it only reduced the risk of getting shingles by 51% and PHN by 67%. In 2017 a new vaccine was approved in the U.S. called Shingrix. This vaccine is a two-injection vaccine with the second shot given 2 to 6 months after the first. This vaccine is recommended for everyone 50 years or older. The big advantage of this vaccine is that is 85-97% effective in preventing both shingles and PHN. For more information about this vaccine you can go to the CDC website by clicking here.
Article contributed by Dr. Brian Wnorowski, M.D.
Getting your eyes dilated can be inconvenient – dilation makes the eyes light sensitive which can make it difficult to read books or use phones and computers for a couple of hours.
So wouldn’t it be great to have another drop to reverse the effects of dilation?
On Dec. 31, 1990, dapiprazole, under the trade name Rev-Eyes, was approved by the FDA and thought to be the answer to all the post-dilation problems. It was marketed for treatment of medically-induced dilation by stimulating pupillary constriction and restoration of accommodative function for reading.
In clinical practice, dapiprazole took between one to two hours to return pupils to pre-dilation size.
Side effects such as stinging upon instillation, conjunctival hyperemia (redness of eye), headache, and a few instances of ptosis (lid drooping), with a possible additional dollar cost to patients, seemed to lessen dapiprazole’s overall clinical benefit.
Reading ability returned in approximately 43 minutes with dapiprazole vs 66 minutes without the drop (Optom Vis Sci 1994 May; 71(5):319-22). The main complaint that people had after using dapiprazole was the conjunctival hyperemia, which lasted more than three hours. The other issue was that dapiprazole was costly, so some practitioners included an additional charge for the reversal of dilation to offset the cost.
The full adverse reaction profile according to Drugs.com is as follows:
"Adverse Reactions: In controlled studies, the most frequent reaction to dapiprazole was conjunctival injection lasting 20 minutes in over 80% of patients. Burning on instillation of dapiprazole hydrochloride ophthalmic solution was reported in approximately half of all patients. Reactions occurring in 10% to 40% of patients included ptosis, lid erythema, lid edema, chemosis, itching, punctate keratitis, corneal edema, browache, photophobia and headaches. Other reactions reported less frequently included dryness of eyes, tearing and blurring of vision."
Currently, Rev-Eyes is off the market. The FDA has stated that Rev-Eyes was not withdrawn from the market for reasons of safety or effectiveness.
At this time, there is nothing available for reversal of dilation. People who get dilated will still need to wear their sunglasses and to put off reading for a couple of hours until the effects of the dilation drops wear off.
Article contributed by Dr. Jane Pan
This blog provides general information and discussion about eye health and related subjects. The words and other content provided on this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
The tears that coat the surface of your eyes have both a liquid and a mucous layer to them. It is normal to have a small amount of mucus in your tear film. But that mucus can significantly increase when the eye gets irritated.
Some of the most common causes of irritation that can make the eye overproduce mucus are:
- Conjunctivitis, which could be caused by an allergy, bacteria, or virus
- Blepharitis, which is an inflammation of the eyelids
- Dry Eye Syndrome
When any of these conditions occur, the eye will begin to make more mucus.
Sometimes the mucous production really is excessive and there is a temptation to keep pulling it out with either your fingers or a cotton swab. DON'T DO THIS--it will just lead to recurring irritation and problems.
Any mucus that gets deposited OUTSIDE the eye on the outer eyelid or on the lashes is fair game for removal. In fact, anything on the exterior of the eyelid or stuck to the eyelashes should be cleaned off. Just don’t reach INSIDE the eyelids.
Every time you go inside the eye to remove mucus, your finger or a cotton swab further irritates the eye and causes it to make even more mucus and you end up with the viscious cycle that we call mucus fishing syndrome.
If you have an acute problem that is causing excessive mucus, you need to try and get the underlying problems treated and under control. That means treating the allergy, blepharitis, infectious conjunctivitis, or dry eye syndrome.
In addition, you need to STOP putting your fingers in your eye and pulling the mucus out. Sit on your hands if you have to--but you have to stop or it is never going to get better.
If you have gone through treatment for the original problem but still find yourself pulling mucus out of your eye, you may need your doctor to try a steroid drop in order to decrease the production and try to help you get out of the habit of putting your fingers in your eyes.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.